Pay in installments of $7.11 with
![]() ,
,
![]() and
and
![]()
Shipping Estimate
USA
- USA
- CAN
- USA
- CAN
Ships within 48 hours · Estimated delivery Aug 12 - Aug 17
For Your Every Summer RSVP, with Code: SUMMER15
Description
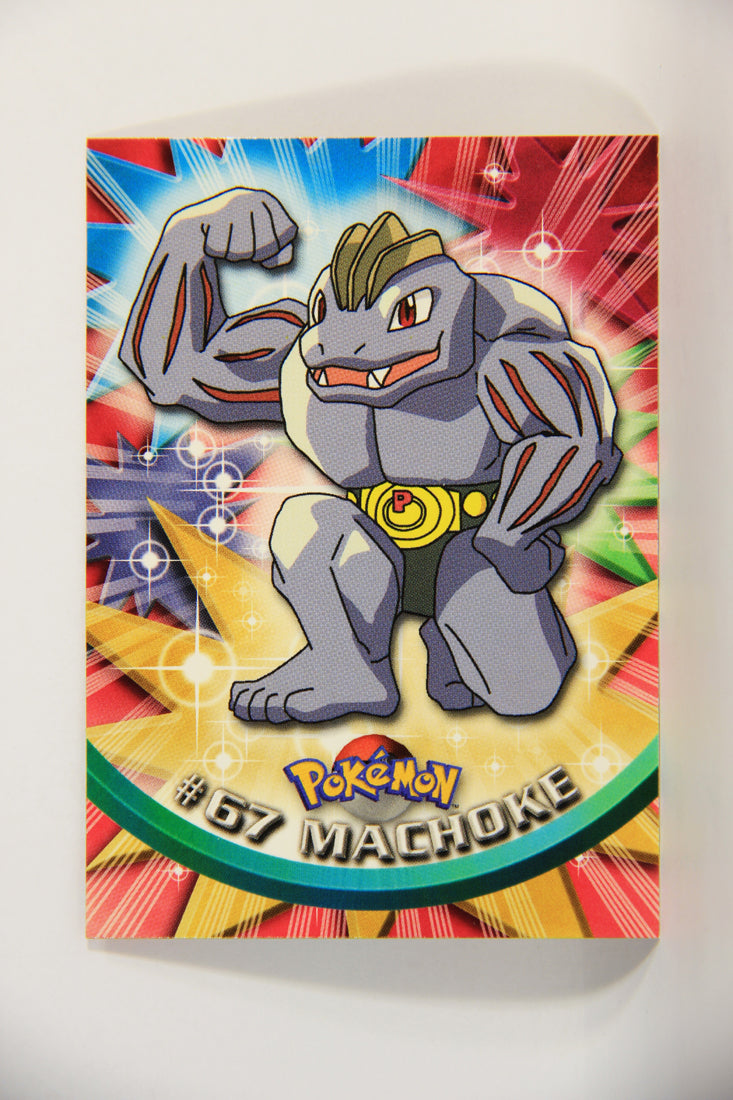
machoke pokemon card value 2016 Pokémon Card Machoke #67 TV Animation Blue Logo 1st Print ENG L015228 – AGS CollectiblesDESCRIPTION TRADING CARDS COLLECTIBLES : Non Sport Trading Cards. BRAND : Topps LANGUAGE : ENG CONDITION : NM ( Near Mint ) This card come from a 85 000 cards collection that has been built from mint card boxes and sealed packs. Although we decided to put this grade and so it might even lead to a higher one. L015228
DESCRIPTIONTRADING CARDS / COLLECTIBLES : Non-Sport Trading Cards.
BRAND : Topps
LANGUAGE : ENG
CONDITION : NM ( Near Mint )
This card come from a 85 000 cards collection that has been built from mint card boxes and sealed packs. Although we decided to put this grade and so it might even lead to a higher one.
L015228
Shipping Notes
- Free Standard Shipping on $100+ Orders to the USA.
- Except Preorder products are shipped in 48 hours.
- Delivery to the USA:
- Standard Shipping : 3-10 business days
- If time is of the essence, please consider selecting expedited delivery for faster service.
Exchange/Return Notes
- We offer a 30-day return/exchange service after receiving.
- Final sale items are not eligible for returns or exchanges.
- To process your return/exchange, please contact us at [email protected]
- Please click here for more details>>> Return & Exchange Policy